A Robot Performed Surgery All By Itself
11:27 minutes
Almost a quarter of all surgeries in the United States use robots. And every one of those robots’ movements in the operating room is controlled by a surgeon. But that might begin to change. Researchers at Johns Hopkins University have trained a robot to do surgery on its own, and it recently completed a portion of a gallbladder surgery on a pig cadaver. The results were published in the journal Science Robotics.
Medical roboticist Axel Krieger joins Host Ira Flatow to discuss how he was able to train this impressive surgical robot.
Keep up with the week’s essential science news headlines, plus stories that offer extra joy and awe.
Dr. Axel Krieger is an Associate Professor in the Department of Mechanical Engineering at Johns Hopkins University.
IRA FLATOW: If you’ve had surgery recently, your surgeon might have been a robot. Yeah, almost a quarter of all surgeries in the US use robots. But don’t be alarmed because every one of the robot’s movements in the operating room is actually controlled by a surgeon.
But there is change in the wind because for the first time, researchers at Johns Hopkins University have trained a robot to do surgery on its own, a portion of a gallbladder surgery on a test pig cadaver. The encouraging results were published this week in the journal Science Robotics.
Joining me now to dissect how he trained the robot to accomplish this feat and what it means for the future of robotic surgery is Dr. Axel Krieger, associate professor in mechanical engineering at Johns Hopkins University, based in Baltimore, Maryland. Welcome to Science Friday.
AXEL KRIEGER: Thank you so much for having me.
IRA FLATOW: You’re quite welcome. Can you walk me through what part of the surgery the robot was able to perform all by itself?
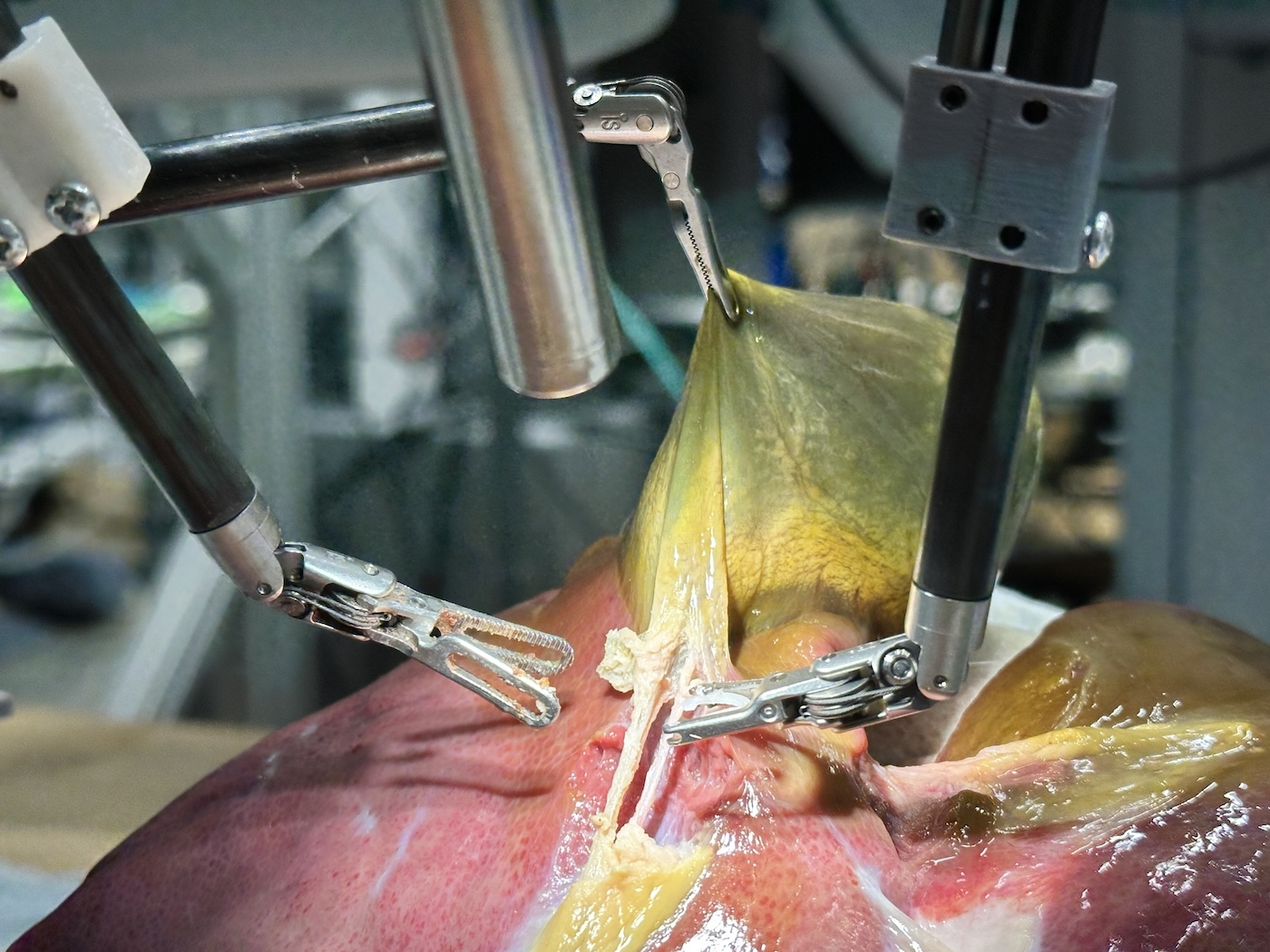
AXEL KRIEGER: Yes. There are about three large portions of gallbladder surgery. The first one is dissecting the gallbladder from the liver bed. The second part– that’s what we really focused on– is the precision at clipping and cutting of the artery and the bile duct.
So this is going in with small, little clippers and identifying where the artery is, placing three plastic clips in it, and then identifying where the bile duct is, then placing three plastic clips in that, and then dissecting between the clips so that the gallbladder then in the third procedural step can be, effectively, removed. And so that’s a very complex, lengthy step and really requires a lot of precision. And there’s a lot of deformation of the tissue and anatomical variations, even between healthy pigs.
IRA FLATOW: Right. So how do you train a robot to do this?
AXEL KRIEGER: We used a technique called imitation learning. We can, effectively, now watch expert surgeons perform these steps and then repeat these steps over and over and then train a network to learn to then reproduce those steps. So we can tie what the robot sees to what the robot should do. So it’s a hierarchical framework that first predicts the right phase of the surgery and then predicts what the robot should do, given the certain video image that the robot sees currently.
IRA FLATOW: What happens if the robot makes a mistake? Is it able to correct itself before it does something really bad?
AXEL KRIEGER: Yeah. The really nice thing that we demonstrated in our study is that our robot is capable to adapt to small, little displacements. So imagine if the clipper doesn’t catch the artery perfectly on the first try. The system automatically recognizes that and then self-corrects.
That’s one way– so self-correction by the robotic systems. And then also, the surgeon would then be the supervisor and could always stop and take over and complete the procedure manual, if necessary. In our study, in eight consecutive pig surgeries, we didn’t need any interventions. But if something unforeseen happens, the surgeon can always intervene and take over.
IRA FLATOW: Right. Were you surprised yourself just how well the robot performed here?
AXEL KRIEGER: Yeah, super exciting result. When we set out on this project, we didn’t expect that we would get to a point where we didn’t need any human intervention. So this was, really, even better than we anticipated.
IRA FLATOW: Let’s talk about getting to that point. How do you get to that point? How big a jump in technology is this new robot from other, older ones?
AXEL KRIEGER: It’s a major step forward. In older systems, we were able to automate maybe one small task, one little step. And now tying these steps effectively together and recognizing small mistakes and then consecutively performing these sub-steps to do a big chunk of a surgical procedure– that’s a huge step forward.
IRA FLATOW: Yeah, because you’ve been designing robots to do this itself for a few years now, right?
AXEL KRIEGER: Absolutely. We published a study in 2022 where we did a step called the anastomosis. So that’s suturing of tubular structures. And so we were able to perform that suturing step. But what’s really exciting now is that we can boost up the success rate. And we have this framework that is more general. So we can train it for all different types of procedures, not just one step. But by adding more data, we can just learn more procedures and really get closer to clinical viability of this technology.
IRA FLATOW: I watched a video you put online of the robot actually doing this work. And I was surprised how well it did it. How does the robot’s work compare to a human surgeon?
AXEL KRIEGER: In our study, we really wanted to demonstrate the feasibility of this technology. So we didn’t do a very thorough evaluation comparing to expert surgeons. We did a small, little comparison to one surgeon and showed that our robot is a bit slower. We ran it quite slow so we can intervene if something happens. But the movement was more smooth compared to the expert surgeon– so really, some early indication that we are getting on par with even an expert surgeon there.
IRA FLATOW: And what about other kinds of surgeries? Now that you’ve had success with this, do you see you’re able to expand to others besides just gallbladder surgery?
AXEL KRIEGER: Yeah. For us, this is a fantastic starting point. Gallbladder surgery was the first surgery that was performed minimally invasively– so has this lighthouse character of a new technique for surgery. So that’s why it’s such a good target. But we are excited to use this technology now for other applications, for other surgeries.
A big one that we are working on right now is precision tumors resection, where it’s so difficult to delineate where the tumor is from the healthy tissue and cutting that out precisely. That is so difficult for surgeons. And we’d really want to use this technology to improve surgical techniques.
IRA FLATOW: I was going to ask you about the benefit of a robot that can do surgery without human intervention. But you’re saying here that in some cases, it can do it better than the surgeon?
AXEL KRIEGER: Yeah, that’s what we are working on. So integrating pre-operative scans, effectively– so seeing where the tumor is on other imaging– and then combining it, effectively, with surgical videos– that’s the next big goal that we’re working on. And that is very hard for human surgeons, to map these things together in their head. And so doing this with a robot, we might be able to even boost expert surgical performance.
IRA FLATOW: Are you saying a robot independent of a surgeon guiding it, or with surgeon supervision?
AXEL KRIEGER: Always surgeon supervision. Our goal is not to replace surgeons. We want to just make the surgery easier and help surgeons work with this rising caseload. We have an aging society, more surgeries needed. And so the individual caseload is doubling in the next 10 years.
So how can we help surgeons with that? How can we do an effective surgery later in the day, when the surgeon might get tired? By helping the surgeon not having to do every part and every little step of every surgery. But then for portions of it, just watch the robot do it. And then intervene, if necessary. That can really improve the effectiveness and the efficiency of surgeries.
IRA FLATOW: A lot of surgeries are done today through lap surgery, laparoscopy, right? Can the robot do that also?
AXEL KRIEGER: Yeah, absolutely. So the big improvement of using surgical robots is making it easier to do laparoscopic surgery, minimally invasive surgery. So traditionally, surgeons had to perform large incisions and work with the organs directly with the hands, guidance directly with the eyes. Now we use cameras and small ports. And we use surgical tools in ports. And the surgical robot that we’re working with is a minimally invasive keyhole surgery robot. And so we can do this procedure minimally invasively, yes.
IRA FLATOW: All right. Now, you know we have listeners who are listening to this. And they’re going to ask, how do I get in on this? How soon might patients see autonomous robots, perhaps this gallbladder surgery, in the operating room?
AXEL KRIEGER: We are super excited to take the next steps and go to do a preclinical study. So demonstrating this in live pig surgeries– that’s our next steps that we are very, very hardworking on right now.
I also see that, similarly to modern cars, where we have some autonomous functions, like brake assist, park assist, those autonomous functions, we see those coming in surgical robotic systems for the next few years. So for example, the FDA approved recently a camera system that can follow the surgery autonomously.
So the camera is moving autonomously, not the surgical tools. And now we can see maybe suction, maybe holding tissue, those things to be coming over the next few years. It’s going to take a while before procedures like gallbladders are implemented clinically and commercially. But we can definitely see the path forward for those.
IRA FLATOW: So what’s your next work here? You were studying this on a pig cadaver, right? Do you ever get to the living, breathing pig section?
AXEL KRIEGER: That’s exactly the next step. So we demonstrated this on pig cadavers. And now we are working very hard to see if we can do this in a living pig. That would be the next step. And then we’d demonstrate that this is safe and effective. Then we can really design a first-in-humans study and work on the regulatory approval for that.
IRA FLATOW: What’s the most challenging part about creating and training these robots?
AXEL KRIEGER: The most challenging part is getting the right training data. So we acquired about 30 different cadaver from butchers and then tested on all different anatomy and variations in the lab to acquire our testing data.
And we also needed to predict how our robot might make small, little mistakes and then add them manually to the training data– so start some procedures with maybe the clipper or the cutter being a little bit misaligned from the target so that we can self-correct them during the procedure. So you become a bit of a robot whisperer. You anticipate mistakes. How could I fail? And then add that to the training data. So that’s probably the most complex part of our work.
IRA FLATOW: We have run out of time. I didn’t get to ask you about how a robot scrubs up for surgery. But that’s for the next time. We can talk about that.
AXEL KRIEGER: Thank you so much. That was fantastic questions.
IRA FLATOW: You’re quite welcome. And come on back when you’re working in a little more in vivo, in live pigs.
AXEL KRIEGER: Absolutely– would love to come back. Thank you so much for your interest and this fantastic interview. I really enjoyed it.
IRA FLATOW: You’re welcome– Dr. Alex Krieger, associate professor in mechanical engineering at Johns Hopkins University in Baltimore, Maryland.
Copyright © 2025 Science Friday Initiative. All rights reserved. Science Friday transcripts are produced on a tight deadline by 3Play Media. Fidelity to the original aired/published audio or video file might vary, and text might be updated or amended in the future. For the authoritative record of Science Friday’s programming, please visit the original aired/published recording. For terms of use and more information, visit our policies pages at http://www.sciencefriday.com/about/policies/
Shoshannah Buxbaum is a producer for Science Friday. She’s particularly drawn to stories about health, psychology, and the environment. She’s a proud New Jersey native and will happily share her opinions on why the state is deserving of a little more love.
Ira Flatow is the founder and host of Science Friday. His green thumb has revived many an office plant at death’s door.