How Scientists Unravel The Mysteries Of The Placenta
17:19 minutes
Here’s a fun fact for your next virtual trivia night: What’s the only organ that we can grow temporarily, and discard after it’s been used? The answer: the placenta.
It may be a disposable organ, but scientists have a tricky time studying it: You can’t poke at it, sample it, or pull it out to see how it works while it’s doing its job of growing a human baby.
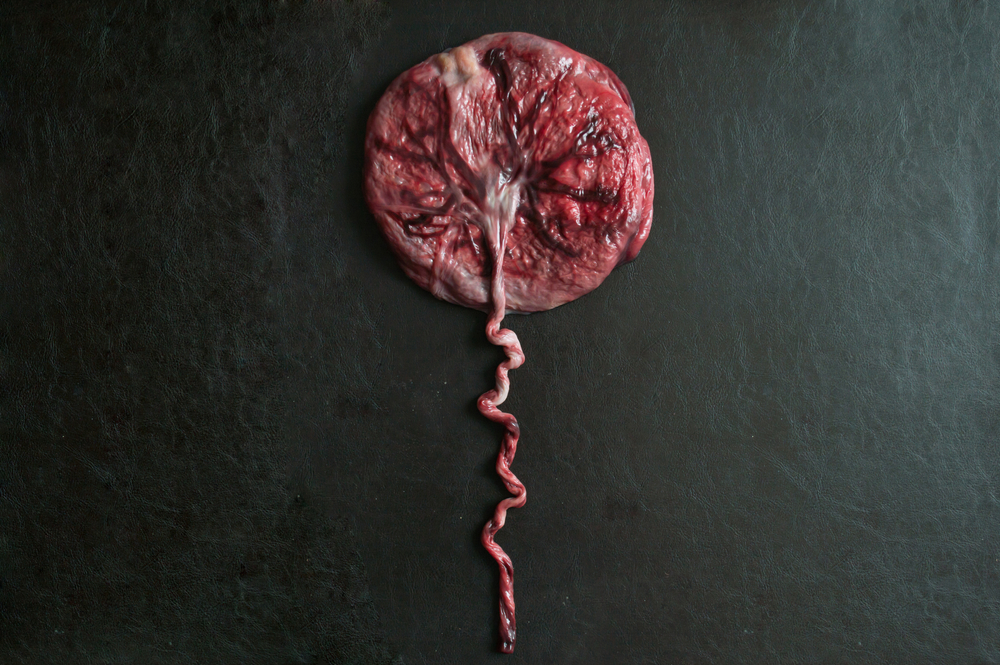
In an effort to understand how this squishy, purplish, pancake-shaped organ performs some of its most important functions, researchers have had to turn to creative techniques. Ann-Charlotte Iverson, professor at the Norwegian University of Science and Technology, and Nicholas Heaton, assistant professor at Duke University, join Science Friday to discuss how the placenta protects a fetus from viral infection and inflammation, and what happens when something goes wrong.
Invest in quality science journalism by making a donation to Science Friday.
Ann-Charlotte Iversen is a professor at Norwegian University of Science and Technology and the Center for Molecular Inflammation Research. She’s based in Trondheim, Norway.
Nicholas Heaton is an assistant professor in the Department of Molecular Genetics and Microbiology at Duke University in Durham, North Carolina.
IRA FLATOW: This is Science Friday. I’m Ira Flatow. Here’s a fun fact for your next trivia contest. What’s the only organ that we can grow temporarily, and discard it after it’s been used? The answer– the placenta. Cool, no? The placenta may be a disposable organ, but scientists can have a tricky time studying this odd-looking afterbirth. Sci Fri’s Katie Feather has more.
KATIE FEATHER: Maybe you’re already grossed out by the word placenta, the way some people shudder at the word moist. If so, think about this. Everyone on Earth was once familiar with the placenta. It shows up at every single person’s birth. On the other hand, maybe you’re really comfortable with the idea of the placenta as a symbol of mystical feminine power. Perhaps you’ve eaten one for its purported health benefits, or buried one as part of a sacred ritual.
So there’s a lot that comes up when people mention this squishy, purplish, pancake-shaped organ that makes growing a human possible. A lot of stories, a lot of symbolism, but not a lot of science. Because when it comes to studying the placenta, scientists are at a disadvantage since you can’t poke at it, sample it, or pull it out to see how it works while it’s doing the job of growing a human baby.
But my next two guests found creative ways around that in their effort to understand how the placenta does one of its most important jobs– protect the fetus– and some ways that can go wrong. Here to explain what they did and to talk about the mysteries of the placenta are my guests.
Dr. Ann-Charlotte Iversen is a professor at the Norwegian University of Science and Technology in the Center for Molecular Information Research in Trondheim, Norway. And Dr. Nicholas Heaton is an assistant professor in the Department of Molecular Genetics and Microbiology at Duke University. Welcome both of you to Science Friday.
NICHOLAS HEATON: Thank you. It’s great to be here.
ANN-CHARLOTTE IVERSEN: Thank you.
KATIE FEATHER: So Dr. Iversen, I want to start with you. Can you take us back to high school biology and remind us what the placenta actually does?
ANN-CHARLOTTE IVERSEN: So the placenta has many functions. To provide the fetus with sufficient nutrition and oxygen, and also remove the waste products from the fetus. In addition, the placenta must protect the fetus from infections. And also the placenta is the setting where it has established a coexistence between these two different individuals, and that’s a big immunological challenge.
KATIE FEATHER: You mentioned that the placenta actually has two sides. One side that connects to the mother with these certain types of cells, and a different group of cells that are on the fetal side. That’s so cool. I didn’t know about that.
ANN-CHARLOTTE IVERSEN: Yeah, that’s true. So when the placenta starts forming, the blastocyst attach to the uterine wall. And then these specialized fetal cells, called the trophoblasts, invade the uterine wall of the mother and they start forming the placenta. And these trophoblasts, they are the cells that meet the mother directly in the uterine wall where these specialized fetal cells sit and interact with maternal cells. And they are also close to the uterine blood vessels that supply the placenta with blood.
KATIE FEATHER: So one reason it’s so hard to study the placenta is because ethically you can’t access it while it’s in use, right?
ANN-CHARLOTTE IVERSEN: Yeah, that’s right. We have to wait until delivery.
KATIE FEATHER: So how do you get around that obstacle when you’re studying the placenta? Tell me how do you get your placenta?
[LAUGHTER]
ANN-CHARLOTTE IVERSEN: So we get our placentas from the cesarean sections, because then we can avoid the stress of labor and delivery on the placenta. So the placenta is delivered and we take samples from the placenta itself. And then to get to that maternal side of the placenta, we do a vacuum suction method where the placenta was sitting in the uterine wall to get access to that tissue that represents the maternal side of the placenta. And we sample these tissues as soon as possible, so that it’s as much like as it was in vivo or in the mother as possible.
KATIE FEATHER: I’m imagining it like when someone is donating an organ, there is a very rapid process of getting that liver, or whatever, to where it needs to go. So how quick is as soon as possible for a placenta?
ANN-CHARLOTTE IVERSEN: So we ask the mother before the cesarean section, so that is set in place. And she will give her consent for us to take out the samples. But ideally, from when the placenta is taken out, we would like to have the sample stored, either frozen or fixated, within half an hour. And that’s a challenge. So we have to have everything set ready for the sampling for each delivery.
KATIE FEATHER: So one of the things that the placenta is doing is helping to protect the fetus from viral infection. Dr. Heaton, how does the placenta do that?
NICHOLAS HEATON: Yeah, I mean, this is a great question. And there’s multiple layers that go into this. I mean, the primary function– the way the placenta keeps pathogens out is just by serving as a barrier. If there are pathogens that are circulating in the maternal blood, these specialized cells that were referred to earlier– these trophoblasts– actually form barriers that stops pathogens from getting across. And that works in the vast majority of cases.
But in addition to the actual pathogen itself crossing the placenta, there’s also this issue of inflammation that needs to be dealt with. And really those are the two ways– at least when we think of it from an infectious disease side, those are the two kind of functions the placenta has to play.
KATIE FEATHER: Yeah. Tell me more about inflammation. That’s the body’s response to a virus. It’s an immune response. So obviously, the mother needs that inflammation response to help combat the virus. But it can be bad for the fetus. So what’s the placenta’s role there?
NICHOLAS HEATON: Yeah. The immunological system here is really complex, because the immune system is basically designed to identify what is self and what is non-self. And the fetus has genetic material from the father and so it already starts out as genetically different than the mother. So there’s already some complex immunological processes at play here.
But it gets more complicated during a maternal infection. Now you have a system, like you just alluded to, where the mother needs to fight off this infection, while at the same time not fight off the developing fetus. And so inflammation is a generic term.
But what the body has to do is identify that there’s a pathogen and then start secreting these inflammatory mediators, which are called cytokines and chemokines, which basically tell the body that there’s a pathogen that has initiated infection and start the process of fighting it off. And then the mechanisms for how that’s controlled– how the antiviral response in the case of a virus infection can do that and preserve maternal health while at the same time avoiding those same processes in the placenta and the developing fetuses is an area of active investigation.
KATIE FEATHER: So you conducted a study where you found that the placenta was good at protecting the fetus against influenza, but not against Zika virus, which is a mosquito-borne virus that causes fetal abnormalities in babies whose mothers contract it. So what did you discover is happening in the placenta with these two viruses?
NICHOLAS HEATON: Yeah. So one of the really interesting questions that our group has been focused on is why is the placenta able to deal with inflammation in some cases and not in others? And so in a study we just completed, we really looked at pathways that can protect the developing fetus from maternal infection caused by influenza virus compared to inflammation after Zika virus infection.
Both of these infections induce similar types of inflammation, but there are key differences in where the virus is replicating. And so the key finding from our study was that there is a key inflammatory pathway to suppress virus replication. And both influenza and Zika virus induce this pathway. But we found a protein that’s able to suppress the activities of the inflammatory type 1 interferon. We used an influenza virus infection system where it works. And so we know the answer for flu.
The question is why isn’t that enough for Zika? And we don’t know the answer to that yet. But we suspect that it has to do with the local concentration of these inflammatory mediators that ultimately are responsible for a lot of the birth defects that we see.
KATIE FEATHER: You didn’t investigate this with SARS-CoV-2, but would you guess the immune response to coronavirus would be more like Zika or more like flu in pregnant women?
NICHOLAS HEATON: Yeah. So the coronavirus is certainly much closer to flu than it is to Zika. And we know that SARS-CoV-2 is not associated at least with severe birth defects like we see after Zika. And so we think it definitely falls much more into the flu side of things. And this GP1 mediated suppression pathway is probably at work protecting the fetus when pregnant women are infected by SARS-CoV-2.
KATIE FEATHER: That’s great. Getting back to that question of how do we even study the placenta, because it’s such a complicated organ doing a very important job and we can’t get to it. So how do you access placentas for your research?
NICHOLAS HEATON: Yeah. So we used a combination of human tissue samples that were collected just like Dr. Iversen describes. But we really took advantage heavily of some animal models of virus infection, because our goal here was to manipulate the inflammatory signaling pathways and see what the effects on the developing fetus would be. Obviously, this is something that you could never do in people.
KATIE FEATHER: What’s the best animal model for placenta research?
NICHOLAS HEATON: Yes, that’s a complicated and difficult question. We used mice in the study because they’re a good model for the pathogens that we were using for the influenza virus and Zika virus. Mice have a different structure to the placenta than humans do. So it’s never a perfect comparison. But we think we can learn enough from these systems and then validate key findings in human tissues to draw these conclusions with high confidence.
KATIE FEATHER: Dr. Iversen, one of the biggest concerns for mothers and their medical providers is the development of preeclampsia during pregnancy. So can you tell us what that is?
ANN-CHARLOTTE IVERSEN: So preeclampsia occurs in 4% to 5% of pregnancies and may lead to severe sickness and even death in both the mother and fetus. So this might pose a serious threat in pregnancy. It’s diagnosed in the late stages by onset hypertension and most often proteinuria in the mother. So preeclampsia starts most often by improper placenta formation and this leads to a dysfunctional and stressed placenta that is characterized by harmful inflammation and oxidative stress.
And as the fetus grows, this dysfunctional placenta sends more and more stress signals to the maternal blood. And this eventually becomes too much of a burden for the mother and she develops the clinical signs– hypertension and proteinuria. So most often, preeclampsia consists of the two components– placental dysfunction and the maternal response.
Also, to add to this, we have no effective treatment of preeclampsia other than delivery of the baby and the placenta. And therefore, preeclampsia is often associated with preterm delivery.
KATIE FEATHER: This is Science Friday. I’m Katie Feather, talking with Dr. Ann-Charlotte Iversen, professor at the Norwegian University of Science and Technology, and Dr. Nicholas Heaton, assistant professor at Duke University, about the mysteries of the placenta.
I have to say when I was going through this most recently, the coronavirus was definitely a concern of mine. But I was terrified of preeclampsia, because everything I read and everything I’d heard suggested that we don’t know why women get it. It just happens.
And then you combine that with some very severe outcomes. Like you said, increased maternal and infant mortality rates, preterm delivery. So it just seemed very terrifying and unknown. So how much do we know about how and why this placental dysfunction occurs?
ANN-CHARLOTTE IVERSEN: So we know something about how this develops. It will start as early as during placenta formation when these trophoblasts invade the uterine wall. Then they participate in remodeling of the uterine spiral arteries. They are being remodeled to wide vessels that will ensure sufficient blood flow to the placenta.
In the early stages of preeclampsia, the invasion of trophoblasts and the remodeling of these vessels doesn’t occur the way it should. And the result is a placenta that gets abnormal blood supply and develops to be a stressed organ. So we know something about the initial phase. But then we have this whole development of this stressed organ, and how it affects the mother, and what parts, and inflammatory and oxidative stress mechanisms that are at play. And there’s a whole lot more to figure out to be able to both treat this disease and also to predict it.
KATIE FEATHER: You mentioned inflammation and I’m seeing a connection between this condition and mediating viral infection, which is what Dr. Heaton was talking about. Given that inflammation seems so disruptive, couldn’t we just treat the inflammation?
ANN-CHARLOTTE IVERSEN: To be able to handle the harmful inflammatory levels that we see in diseases, such as preeclampsia, we need to understand where is the line between harmful and normal and what types of inflammatory activation is mostly causing the harmful inflammation we see in these. So in our study we relate to the similarities between cardiovascular disease and preeclampsia. We know that in atherosclerosis, cholesterol crystals induce a very potent inflammation and promote development of atherosclerotic lesions in the blood vessels.
And what we did reveal indeed is that there are cholesterol crystals present at the maternal side of the placenta. And we know that preeclampsia and cardiovascular disease have so many similarities. So this– it makes sense that the same consequence of too much cholesterol accumulation in the tissue leads to production of these cholesterol crystals, which are potent, harmful, and just a sort of inflammation.
KATIE FEATHER: And Dr. Heaton, I know the placenta isn’t the focus of your research all the time. But you’ve waded into these waters now. So do you have any future plans to continue studying the placenta?
NICHOLAS HEATON: Yeah, absolutely. I mean, like I said, I think– like a lot of scientific questions, the more we learn, the more we realize we don’t know. One of the things that we’re most excited about following up now is in our previous studies we’ve identified some pathways that are important, and we know that they’re important because we broke them and we made things worse for pregnancy.
And really what we want to do now is look at the flip side. Now that we know these pathways are important, instead of breaking them, can we make them work better. Can we make them stronger to potentially protect fetal health under conditions where things aren’t working correctly and we’re seeing things like birth defects.
KATIE FEATHER: I want to thank you both for taking on the task of describing this research for our listeners today, because it seems very complicated. So you guys both did an amazing job. Why is it so hard to talk about this type of science?
[LAUGHTER]
ANN-CHARLOTTE IVERSEN: Now that’s a good question. It’s very motivating to be working in this field, but it’s very complex and there is a lot of processes that occur at the same time. And we have to approach it from our different platforms and try to work together to figure out this complex setting.
NICHOLAS HEATON: I mean, the placenta wasn’t even particularly well– I mean, it was referred to as afterbirth. It’s just something that happens after the birth. So when you want to talk about this, you have to start with here’s what the placenta is, here’s why it’s cool, here’s the problem, and then here’s what we found.
KATIE FEATHER: Well, thanks so much again for joining us.
NICHOLAS HEATON: Yeah, thank you. It was great chatting.
ANN-CHARLOTTE IVERSEN: Thank you for having me.
KATIE FEATHER: Dr. Ann-Charlotte Iversen is a professor at the Norwegian University of Science and Technology at the Center for Molecular Information Research in Trondheim, Norway. And Dr. Nicholas Heaton is an assistant professor in the Department of Molecular Genetics and Microbiology at Duke University. For Science Friday, I’m Katie Feather.
Copyright © 2021 Science Friday Initiative. All rights reserved. Science Friday transcripts are produced on a tight deadline by 3Play Media. Fidelity to the original aired/published audio or video file might vary, and text might be updated or amended in the future. For the authoritative record of Science Friday’s programming, please visit the original aired/published recording. For terms of use and more information, visit our policies pages at http://www.sciencefriday.com/about/policies/
Katie Feather is a former SciFri producer and the proud mother of two cats, Charleigh and Sadie.